A study to compare the effectiveness of diaphragmatic training and chin tuck exercises among Physiotherapy, Nursing and Degree students with forward neck posture on craniovertebral angle using photogrammetry: Dr.Kurapati Madhava Reddy1, Ph.D., D.Sc., Professor & Principal, Sri Lakshmi Institute of Medical Sciences College of Physiotherapy, Kavali, Andhra Pradesh, India.; Dr.S.Gopikannan,2 B.P.T., Professor & Vice Principal, Sri Lakshmi Institute of Medical Sciences College of Physiotherapy, Kavali, Andhra Pradesh, India.
Background:
Throughout the world, young adults are more prone on using technologies which can be in many forms such as desktop computers, laptops and smart phone (Mosallaiezadeh S et al 2022) Since, these gadgets are appealing and are available in a number of varieties, many people especially college students and teenagers using them for a longer period of time are suffering from musculoskeletal issues (Dareh-deh HR et al 2022).
Abnormal posture causes some muscles to shorten and some muscles to lengthen simultaneously, which leads to muscular imbalance. It exerts more strain on ligaments, muscles, and other body parts and leads to various pathological conditions (Singh V et al 2020). Usually along with abnormal posture, such as rounded shoulders and a forward neck posture (FNP), psychological issues like anxiety, headaches, insomnia, depression, lack of sleep and exhaustion can also occur (Arooj A et al 2022). Literature has reported a number of risk factors for prevalence of forward neck posture in young adults, in which, constant neck pain is at the top of the list. The prevalence rate of FNP worldwide exceeds 66% and it occurs at various severities, i.e., slight, moderate, or severe. Following the study, it was estimated that 1-year incidence of neck pain has ranged from 10.4% to 21.3% which may further lead to forward neck posture (Arooj A et al 2022).
The Forward neck posture is the most common deviation from normal curvature in cervical spine and it is associated with poor habitual neck posture that is defined by hyperextension of the upper cervical vertebrae and forward translation of the cervical vertebrae. FNP increases compressive loading on tissues in the cervical spine, particularly the facet joints and ligaments. Studies have reported that symptoms including neck pain, headache, temporomandibular pain and musculoskeletal disorders related to FNP (Singh V et al 2020). The Forward neck Posture not only affects the functional movement of neck but also the act of breathing. Forward neck Posture affects the scapular muscles and the major core muscles including transverse abdominus in anterior, multifidus in posterior, the pelvic floor in inferior and diaphragm in the superior which will lead to instability of thoracic spine and alters the mechanics of chest expansion. The excessive Forward neck Posture can predominantly affect the main respiratory muscle i.e., diaphragm, because of increased thoracic kyphosis and cervical lordosis (Singh V et al 2020).
The diaphragm is a muscle with a dome form that is essential for breathing and postural stability. In short, altering the diaphragm’s pattern of movement can cause hypoxia, respiratory alkalosis, decreased lung volume, and increased irritability of the central and peripheral neurological systems phone (Mosallaiezadeh S et al 2022). Diaphragm is located between the thorax and abdomen and has extensive and complex fascial connections to surrounding organs, muscles, and bones. Few studies showed that applying diaphragmatic training helps to improve functions in patients with low back pain (Koseki T et al 2019).
Breathing biomechanics have been described with respect to expansion of the abdomino- thoracic region during inspiration at rest. Apical or upper costal breathing occurs when superior thoracic expansion exceeds the abdominal and lateral costal expansion. The tonic phase of diaphragm coordinates with the breathing cycle and the phasic phase coordinates with the postural stabilization of the trunk followed by complete flattening of the diaphragm muscle. In Forward neck posture, muscle mal adaptation, and when greater muscle activity is needed to maintain postural stability, the diaphragm flattens. However, its excursion during breathing is smaller. In a situation like this individual usually hold their breath to increase postural stabilization and diaphragm is primarily activated for stabilization function (Singh V et al 2020).
Furthermore, a significant relationship is observed between increased Forward neck Posture and decreased respiratory muscle strength. It is advised to assess and alter breathing patterns as part of the initial line of treatment plans for patients with Forward neck Posture, since diaphragmatic training is a safe, non-invasive technique that helps people become aware of their posture and breathing pattern (Mosallaiezadeh S et al 2022). Common treatment approaches to improve Forward neck posture includes stretching of a specific group of muscles, strengthening of specific muscles, posture re-education techniques, workplace modifications, biofeedback techniques and application of external appliances to maintain the posture through postural education like respiratory exercise, ergonomic office modification. Due to mid-cervical instability in Forward neck posture, neck stabilization exercises play a major role in Forward neck posture management (Koseki T et al 2019).
Chin tuck exercise has been traditionally prescribed to manage this condition. The chin tuck exercise is designed to counteract chronic forward neck posture by strengthening the deep neck flexor muscles (Koseki T et al 2019). This helps to improve slouched posture, helping to bring the head and upper back backwards restore cervical alignment, and increase the craniovertebral angle (CVA), thereby improving postural control and reducing neck strain settings (Ahmed Iqbal Z et al 2013). Studies have shown that neck pain is treated using McKenzie chin tuck exercise, one of the Deep Cervical neck Flexor exercises, as an effective therapeutic exercise by demonstrating its effectiveness in subjects with Forward neck posture. The current therapy approaches, which included cervical stabilization exercises, thoracic muscle stretching and strengthening activities, and electromyography biofeedback training, has positive improvements on correcting Forward neck posture but the effects last only for short – term. Long term effects are still unclear. Ignoring the diaphragm’s role could be showed as one of the reasons for the weak long-term evidence. However, the physiology of how diaphragmatic training has direct influence on forward neck posture is still unclear (Koseki T et al 2019).
Craniovertebral angle (CVA) is a reliable and objective measure used to assess the severity of forward neck posture (FNP). A decreased CVA indicates greater postural deviation, often linked to neck pain and musculoskeletal imbalance. Photogrammetry requires capturing photographs in a standardized manner. Then, photographs are digitized for further analysis using a computer software. Its ease of use and accuracy, especially with tools like Kinovea, make it a valuable tool for evaluating posture and monitoring treatment outcomes in both clinical and research settings (Ahmed Iqbal Z et al 2013).
The aim of this randomized clinical trial was to compare the effects of diaphragmatic training and chin tuck exercises on forward neck posture (FNP) among students. Previous literature has shown that forward neck posture alters cervical spine alignment, impairs respiratory function, and increases the risk of musculoskeletal pain (Koseki T et al 2019, Kevin Triangto et al 2020). Traditional interventions focus on strengthening deep cervical flexors through chin tuck exercises, manual therapy, and ergonomic modifications (Arooj A et al 2022, Goosheh M et al 2019, Katherine Harman CLHK et al 2005). However, emerging evidence supports the integration of diaphragmatic breathing techniques, which not only influence respiratory efficiency but also promote postural control through core stabilization (Mosallaiezadeh S et al 2022, Dareh-deh HR et al 2022, Fathollahnejad K et al 2019) The current treatment landscape is gradually shifting toward combining biomechanical and respiratory interventions to address FNP more holistically.
The Forward neck Posture not only affects the functional movement of neck but also the act of breathing which has a negative effect on chest expansion. Due to loss of strength in neck muscles, instability of cervical spine occurs that alters the mechanics of chest expansion. Previous studies have shown that diaphragmatic training combined with therapeutic exercises showed increased effect when compared to therapeutic exercises alone. Hence the need arises to know the effect of diaphragmatic training alone compared to chin tuck exercises on Forward neck Posture and this study is undertaken to gather critical information about the potential benefits of including diaphragm in planning treatment for postural correction in patients with Forward neck posture.
Aims & Objectives:
The aim and objectives of the study was to compare the effect of Diaphragmatic training and chin tuck exercises among students with forward neck posture on craniovertebral angle using photogrammetry.
Method:
A Randomized clinical Trial was conducted on Physiotherapy, Nursing and Degree Students with Forward neck posture through Randomized Sampling on 44 Subjects who met the inclusion criteria for a period of 6 months. The approval the study was obtained from the ethical and research committee of Sri Lakshmi Institute of Medical Sciences College of Physiotherapy, Kavali and the purpose of the study was explained to the participants and written informed consent was taken from the subjects who are the students of Sri Lakshmi Institute of Medical Sciences College of Physiotherapy, Sri Lakshmi Institute of Medical Sciences College of Nursing and Sri Sai Degree College,
Kavali and all the study subjects are allotted into either Group A or Group B based on the inclusion and exclusion criteria. CVA (Craniovertebral angle) was taken with the camera was placed perpendicular to the sagittal plane with the markers were placed on tragus of the ear and spinous process of C7 and the CVA was evaluated between the line connecting the tragus, the spinous process of C7, and a horizontal line passing through the C7 as a pre-test measure along with other demographic details.
Subjects in Group A received diaphragmatic training and Group B received chin tuck exercises for 5 days a week, for 4 weeks. All the variables were measured as pretest during the 1st and as post-test during 20th session and the data was analysed and interpreted.
The subjects in Group A performed diaphragmatic breathing exercises in crook lying as 2 sets of 6 – 8 repetitions with 1minute break twice a day for 30minutes, gradually increasing the intensity; while holding 2.5 kg on the abdomen in the first 5 sessions followed by 5 kg in the second 5 sessions. Participants performed 3 sets with 10 repetitions at a ratio of one second of inspiration to two seconds of expiration, three sets of 15 repetitions at a ratio of two seconds of inspiration to four seconds of expiration, and three sets of 20 repetitions at a ratio of three seconds of inspiration to six seconds of expiration. The rest between each repetition was 60 seconds. These exercises were performed 5 sessions per week for 4 weeks.
Subjects in Group B received Chin tuck exercise and based on progression to activate deep neck flexors asking the participant to sit on a chair tucking their chin posteriorly and inferiorly while touching it and hold this position for 10 seconds and followed by a 10 seconds’ break. It was repeated 10 times and the subjects were instructed to complete 3 sets of 12 repetitions of the strengthening exercises and held for 30 seconds each with 5 repetition per week. These exercises were performed 5 sessions per week for 4 weeks.
The outcome of the study was measured by using Photogrammetry to assess FHP which is reliable (r =0.94) and sensitive. Then, sagittal plane photos were taken by the digital camera from each side and saved to a computer for further analysis of CVA.
The data collected and all the variables and its characteristics were described using tables and graphs in excel sheet for analysis. Descriptive analysis was done by finding mean and standard deviation of all the grouped variables as mentioned in the results. The data was then subjected to test of normality. Data is not normally distributed, inferential analysis was carried out by non-parametric tests. The confidence interval for the tests was kept at 95%. Mann Whitney test was used to compare the outcomes between the two groups and Wilcoxon Signed Rank test was used to compare the outcomes within the same group pre and post intervention.
Results:
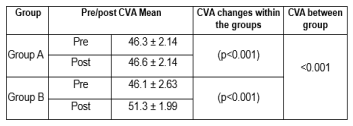
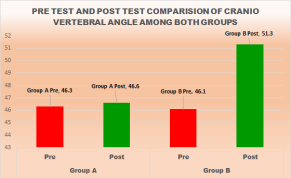
The Statistical analysis of CVA in both the groups indicate that, both Group A and Group B showed statistically significant improvements in craniovertebral angle (CVA) after the intervention (p < 0.001). The within- group effect size was 1.00 for Group A, indicating a moderate effect, and 2.55 for Group B, indicating a strong effect. The between-group comparison also showed a statistically significant difference (p <
0.001), suggesting that the intervention in Group B was more effective in improving CVA and it has been supported by the studies by Mosallaiezadeh S et al 2022, Dareh deh HR et al 2022 that the chin tuck exercise is a targeted intervention designed to
activate and strengthen the deep cervical flexor muscles, primarily the longus colli and longus capitis, which play a critical role in cervical spine stability and postural alignment. In individuals with forward neck posture (FNP), these deep stabilizers are often inhibited or weak, while superficial muscles such as the sternocleidomastoid and anterior scalene are overactive, contributing to muscle imbalance and postural deviation. Chin tuck exercises involve gently retracting the chin
towards the throat without cervical extension, which facilitates isometric activation of deep neck flexors and correction of anterior head displacement (Singh V et al 2020). The repeated activation of these muscles enhances neuromuscular control, proprioception, and endurance, ultimately contributing to improved craniovertebral angle and spinal alignment (Arooj A et al 2022).
Studies by Dareh-deh HR et al 2022, Fathollahnejad K et al 2019 shown that chin tuck exercises lead to a significant improvement in forward head posture by increasing the craniovertebral angle and reducing compensatory activity in superficial neck muscles. Furthermore study by Mosallaiezadeh S et al 2022, Arooj A et al 2022 shown consistent practice contributes to reduced cervical muscle strain and enhanced sensorimotor control, making chin tuck a highly effective and non-invasive strategy in the management of FNP among young adults and students, and this aligns with the current study’s findings, where participants in the chin tuck group demonstrated marked improvement in posture, suggesting the effectiveness of this neuromuscular retraining approach in addressing posture-related dysfunction.
The Craniovertebral Angle (CVA) was used as the primary outcome measure in this study to assess the severity and improvement of forward neck posture. CVA is a reliable, valid, and non-invasive method that quantifies head posture by measuring the angle formed between a horizontal line through the C7 spinous process and a line to the tragus of the ear (Mosallaiezadeh S et al 2022). A decreased CVA indicates a more pronounced forward head posture, making it an ideal marker for postural
changes. It has been shown to correlate well with neck pain, muscle imbalance, and postural deviation (Dareh-deh HR et al 2022). In this study, CVA was essential for objectively comparing the effects of diaphragmatic training and chin tuck exercises, providing a measurable and reproducible indicator of postural correction
This study was designed as a randomized clinical trial to compare the effects of diaphragmatic training and chin tuck exercises on forward neck posture among students. A clinical trial was appropriate because it involved the active administration of therapeutic interventions and the prospective measurement of outcomes, specifically the craniovertebral angle. The randomized design minimized bias and ensured equal distribution of confounding variables between groups, thus increasing the validity of the findings. Unlike observational or non-randomized control trials, this approach allowed for a cause-effect relationship to be established between the interventions and postural improvements, which is essential in physiotherapy-based posture correction studies.
Both diaphragmatic training and chin tuck exercises resulted in significant improvements in forward neck posture, as evidenced by changes in craniovertebral angle. Diaphragmatic training likely contributed to improvement by enhancing core stability, improving postural control, and reducing accessory muscle overuse in the neck and shoulders. This can lead to better postural alignment indirectly over time. However, chin tuck exercises showed greater effectiveness, likely due to their direct targeting of the deep cervical flexor muscles, which play a critical role in maintaining proper head and neck posture. The biomechanical realignment promoted by chin tucks, along with immediate proprioceptive feedback and neuromuscular re-education, makes them more efficient in correcting forward head
Chin tuck exercises demonstrated a more pronounced improvement in forward neck posture within the short-term 4-week intervention, primarily due to their direct activation of deep cervical flexor muscles and immediate impact on postural alignment. In contrast, diaphragmatic training also showed short-term effects; however, its benefits are likely to become more significant with prolonged application. By enhancing core stability, reducing accessory muscle overuse, and improving breathing efficiency, diaphragmatic training may contribute to sustained postural correction over time. Therefore, diaphragmatic training holds promise as a valuable long-term strategy in comprehensive posture rehabilitation.
Conclusion:
From the outcome results of the study, it is concluded that both diaphragmatic training and chin tuck exercises led to significant improvements in craniovertebral angle (CVA) among students with forward neck posture both the groups. However, chin tuck exercises demonstrated a greater and more clinical improvement in CVA compared to diaphragmatic training. This suggests that chin tuck exercises may be a more effective intervention for correcting forward head posture in this population.
Keywords:
Diaphragmatic breathing, chin tuck exercise, forward neck posture, craniovertebral angle.
References:
1. Ahmed Iqbal Z, Rajan R, Ahmed Khan S, Alghadir AH. Effect of Deep Cervical Flexor Muscles Training Using Pressure Biofeedback on Pain and Disability of School Teachers with Neck Pain. J Phys Ther Sci. 2013 Jun 25;25(6):657–61.
2. Anbupriya Sureshbabu M, Nishanth H, Aishwarya A. Immediate Effect of Chin Tuck Exercises on Craniovertebral Angle and Shoulder Angle Among Collegiates with Forward Head Posture. Biomed Pharmacol J. 2021;14(4):2295–8.
3. An HJ, Kim AY, Park SJ. Immediate effects of diaphragmatic breathing with cervical spine mobilization on the pulmonary function and craniovertebral angle in patients with chronic stroke. Medicina (Kaunas). 2021 Aug 16;57(8):826.
4. Arooj A, Aziz A, Khalid F, Iqbal MH, Ashfaq HB. Forward Head Posture in Young Adults: A Systematic Review. Archives 2022: Volume 03 Issue 01 (Jan-June 2022)
5. B Zachovajeviene , L Siupsinskas , P Zachovajevas , Z Venclovas , D Milonas : Effect of diaphragm and abdominal muscle training on pelvic floor strength and endurance: results of a prospective randomized trial: Sci Rep . 2019 Dec 16;9(1):19192.
6. Dareh-deh HR, Hadadnezhad M, Letafatkar A, Peolsson A. Therapeutic routine with respiratory exercises improves posture, muscle activity, and respiratory pattern of patients with neck pain: a randomized controlled trial. Sci Rep. 2022 Mar 9;12(1):4149.
7. Farzaneh Haghighat, Razieh Moradi, Mohammadreza Rezaie, Nastaran Yarahmadi, Farahnaz Ghaffarnejad : Added value of diaphragm myofascial release on forward head posture and chest expansion in women with symptomatic forward head posture: A randomized controlled trial : Journal of Bodywork and Movement Therapies .Volume 45, December 2025, Pages 645-651
8. Goosheh M, Shafizadegan Z, Rezaieian ZS, Salamehzadeh F, Baharlouei H. Comparing the immediate effect of chin tuck and turtle exercises on forward head posture: A single blind randomized clinical trial. Polish Ann Med. 2019;26(1):8–13.
9. Kang JI, Jeong DK, Choi H. The effect of feedback respiratory exercise on muscle activity, craniovertebral angle, and neck disability index of the neck flexors of patients with forward head posture. J Phys Ther Sci. 2016 Sep;28(9):2477-2481.
10.Kang NY, Im SC, Kim K. Effects of a combination of scapular stabilization and thoracic extension exercises for office workers with forward head posture on the craniovertebral angle, respiration, pain, and disability: A randomized controlled trial. Turk J Phys Med Rehabil. 2021 Sep 1;67(3):291-299
11.Katherine Harman CLHK, Butler H. Effectiveness of an Exercise Program to Improve Forward Head Posture in Normal Adults: A Randomized, Controlled 10- Week Trial. J Man \& Manip Ther [Internet]. 2005;13(3):163–76.
12.Kevin Triangto, Siti Chandra Widjanantie, Nury Nusdwinuringtyas. Biomechanical Impacts of Forward Head Posture on the Respiratory Function. Indones J Phys Med Rehabil. 2020 Oct 21;8(02):50–64.
13.Kiana Fathollahnejad , Amir Letafatkar , Malihe Hadadnezhad : The effect of manual therapy and stabilizing exercises on forward head and rounded shoulder postures: a six-week intervention with a one-month follow-up study : BMC Musculoskelet Disord. 2019 Feb 18;20(1):86.
14.Koseki T, Kakizaki F, Hayashi S, Nishida N, Itoh M. Effect of forward head posture on thoracic shape and respiratory function. J Phys Ther Sci. 2019;31(1):63–8.
15.Menon V V., Baba M, Pavankumar, Suresh S. Effects of Diaphragmatic Training on Posture and Stability in Asymptomatic Subjects: A Randomized Clinical Trial. Indian J Physiother Occup Ther. 2020 Feb 27.
16.Mosallaiezadeh S, Bashardoust Tajali S, Shadmehr A, Attarbashi Moghadam B. Effects of Combining Diaphragmatic Exercise with Physiotherapy on Chronic Neck Pain: A Randomized Clinical Trial. Journal of Modern Rehabilitation. 2023;17(1):83-92.
17.Preeti K, Ahmed N, Vrushali B, Shruti G, Professor A, Khot P. Effect of Chin Tuck Exercise with Pectoralis Muscles Stretching Exercise v/s Chin Tuck Exercise with Scapular Retraction Strengthening Exercise on CVA, SA And Active Cervical ROM in Young Adults Patients in Text Neck Syndrome – A Randomized Clinical Trial. VIMS J Phys Ther 2025 Jul 14];6(1):3–11.
18.Puntonglang P. The effect of diaphragm manipulation on neck pain patients with forward head posture: case study. 2020.
19.R Core Team (2024). R: A Language and environment for statistical computing. (Version 4.4) [Computer software].
20.Sartori R, Barbi E, Poli F, Ronfani L, Marchetti F, Amaddeo A, et al. Respiratory training with a specific device in cystic fibrosis: A prospective study. J Cyst Fibros. 2008 Jul;7(4):313–9.
21.Triangto K, Widjanantie SC, Nusdwinuringtyas N. Biomechanical impacts of forward head posture on the respiratory function. Indones J Phys Med Rehabil. 2020;8(2):50– 64.
22.Vikramjit Singh, Sutantar Singh, Kavita Kaushal: Effect of Exercise Program on Forward Head Posture and Chest Expansion in Students of Adesh University : Int J Heal Sci Res : Year: 2020 | Month: March | Volume: 10 | Issue: 3 | Pages: 168- 171.
23.Youssef AR. Photogrammetric Quantification of Forward Head Posture is Side Dependent in Healthy Participants and Patients with Mechanical Neck Pain. International Journal of Physiotherapy, 3(3), 326–331.