By
Prof. Dr. Sir A. R. Samiullah & Dr. Anees Fathima, Dr.Surendra H.Patil & Dr.Ummer Pangattil
President
National Institute of Alternative Medicine System (NIAMS)
Federation of Acupuncture Systems and Therapy Board (FAST Board)
Bangalore, Karnataka, India.
Abstract
1. Findings In this randomized clinical trial involving 32 patients at Nature’s Wellness Centre Bangalore, Karnataka, India. with poststroke motor aphasia and Childhood Apraxia of Speech those who received 6 weeks of acupuncture treatment with up to 6 months of follow-up showed significant improvements in language function, quality of life, and neurological impairment.
2. Design, Setting, and Participants:
Randomized controlled clinical trial conducted across 3 tertiary Centers in India from October 15, 2019, to October 15, 2025. A total of 32 patients (aged 40–70 years) with first-time ischemic stroke and Aphasia.
Effects of Acupuncture in Post Stroke Aphasia
Post Stroke Aphasia (PSA) is a language disorder that affects about one-third of stroke patients, and many continue to have speech and communication problems for a long time. PSA often leads to reduced social activity, depression, anxiety, tiredness, and poor concentration, which greatly lower the quality of life.
The main cause of PSA is brain cell damage after stroke, which destroys normal nerve connections. Recovery depends on Neuroplasticity—the brain’s ability to form new neural pathways and reorganize itself. This recovery happens in two ways:
1. Repair and reorganization of the remaining neural networks in the damaged area. 2. Compensation by nearby brain tissues or the opposite (healthy) side of the brain.
Acupuncture helps improve nerve repair by enhancing neuroplasticity. It is safe, affordable, and effective for PSA treatment. According to Traditional Chinese Medicine (TCM), acupuncture balances Zang and Fu, clears meridians, and restores energy flow. Therefore, it is widely used as a supportive and long-term therapy to help stroke patients recover language and brain function.
Cause of PSA:
1. Poststroke aphasia (PSA) is mainly caused by infarction in brain regions supplied by the middle cerebral artery (MCA), which are responsible for language function.
2. Conditions like hypertension and ischemia lead to arterial blockage, reduced blood flow, and neuron death, damaging language areas.
Pathophysiology:
1. Ischemia reduces ATP production, causing dysfunction in Na⁺/K⁺ and Ca²⁺ pumps, leading to excess calcium, excitotoxicity, and irreversible neuron damage.
2. These events disrupt nerve communication and cause further degeneration of connected neurons.
3. Neuroinflammation and edema worsen injury and break language-related neural networks.
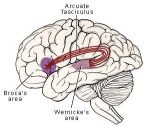
Brain Structures Involved:
PSA primarily affects the left hemisphere language network, including the Broca area, Wernicke area, and Arcuate Fasciculus (AF).
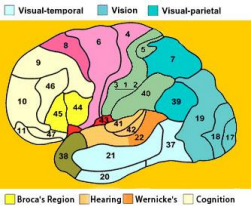
Damage to:
1. Broca area → poor speech fluency – Broca’s area of Brain -Number 44,40.
Brodmann Area: 40
Supramarginal gyrus
Broca’s area Connects
Broca’s and Wernicke’s
Areas 44 and 45 (frontal
Connects Broca’s and Wernicke’s areas (language pathway)
lobe)
Brodmann Areas Connected: 22 ↔44, 45
2. Wernicke area → poor understanding and expression
– Wernicke area of Brain -Number 22,47
3. AF → difficulty repeating words or sentences.
Role of Neurotransmitters and Receptors:
1. After stroke, glutamate becomes overactive, causing excitotoxicity through AMPA and NMDA receptors, leading to neuronal injury.
2. Dysregulated glutamate signaling disrupts subcortical communication, contributing to language processing deficits.
Overall Concept:
1. PSA arises from a combination of vascular damage, cellular energy failure, excitotoxicity, inflammation, and network disconnection in the brain’s language system.
2. Understanding these mechanisms helps guide targeted rehabilitation and neuroplasticity-based therapies such as acupuncture.

The transmission of glutamate. Glutamate
mainly acts on glutamate receptors [AMPAR,
NMDAR, kainic acid receptor (KAR), and
metabolotropic glutamate receptors (mGluR)].
Commonly, glutamate receptors are involved in
synaptic plasticity [long-term potentiation
(LTP)/long-term depression (LTD)] and the
transmission of excitatory neurotransmitters. After stroke, ischemia and hypoxia of the brain will lead to excessive activation of glutamate receptors, causing Ca2+ influx, and increased intracellular Ca2+ concentrations cause excitotoxicity and cytotoxic effects.
Regulation of Glutamate Receptors
Acupuncture has been shown to modulate glutamate receptor activity, including AMPA receptors (AMPARs), NMDA receptors (NMDARs), metabotropic glutamate receptors (mGluRs), and kainate receptors (KARs). Following a stroke, excessive activation of these receptors results in calcium (Ca²⁺) overload and excitotoxicity, ultimately leading to neuronal injury. Acupuncture helps restore balance in receptor activity, thereby reducing excessive Ca²⁺ influx and preventing neuronal apoptosis.
Neuroprotection and Synaptic Stability
Both AMPAR and NMDAR receptors play crucial roles in learning, memory, and synaptic plasticity. Acupuncture may contribute to the stabilization of these receptors, preventing excitotoxic damage to gray and white matter structures, including glial cells, axons, and myelin sheaths. By maintaining synaptic integrity and neural connectivity, acupuncture supports the efficient transmission of language-related information across cortical and subcortical regions, promoting functional recovery and neuroprotection after cerebral injury.
HOW ACUPUNCTURE IMPROVES POST STROKE APHASIA
Improved Cerebral Blood Flow and Ischemia Reduction
Acupuncture enhances local and systemic circulation, improving oxygen and nutrient delivery to ischemic brain tissue. This increased blood perfusion helps reduce infarct size and promotes functional recovery of the affected brain regions involved in speech and comprehension. Promotion of Neural Reorganization
Acupuncture stimulates residual neurons around the lesion and in the contralateral hemisphere, promoting compensatory neural network reorganization. This helps restore communication between language areas (Broca, Wernicke, and arcuate fasciculus) and rebuilds functional pathways for speech production and understanding.
Reduction of Neuroinflammation and Cellular Stress
By improving microcirculation and reducing inflammatory responses after ischemia, acupuncture may limit secondary brain injury, support metabolic recovery, and preserve neuronal viability in both damaged and surrounding regions.
Acupoints Commonly Used in PSA and Their Functions

Yamen (GV15) Functions: Clears the mind, benefits speech, and assists in recovery from aphasia.
Fengfu (GV16) Functions: Improves brain circulation and relieves speech blockages.
Lianquan
(CV23) Functions: Regulates tongue

Shuigou (GV26) Functions: Awakens consciousness, restore s brain function, and supports speech recovery. and speech functions; clears obstruction in the throat region.


Jinjin & Yuye (EX-HN12, EX-HN13) Haiquan
Functions: Dredges meridians, promotes Qi and blood flow, and improves tongue movement and articulation.

Zhaohai (KI6)
Functions: Benefits the throat and speech; supports nervous system recovery.

Sanyangluo (TE8)
Functions: Activates speech-related brain regions and regulates mental function.


Daling (PC7)
Functions: Activates language related Brodmann areas (22, 40, 44, 47); enhances comprehension and speech.
Tongli (HT5)
Functions: Stimulates multiple language-related brain regions; regulates hormones and Qi for better speech recovery.

multiple language-related brain regions; regulates hormones and Qi for better speech recovery.
GB 4 – Hanyan,GB 5 – Xuanlu ,GB 6 – Xuanli Functions: Regulates 1st Speech Area ,2nd speech Area & 3rd Speech Area.
Scalp Acupuncture Therapy
The lower 2/5 of the anterior oblique line of vertex-temporal
MS 6 and anterior temporal line MS 10 will be the needling
sites. The anterior oblique line of vertex-temporal, which
links EX-RN 1 to GB 6 (Xuan li), is on the temporal side of the
head and obliquely passes
through the bladder and
gallbladder meridians. The
anterior temporal line is a part of
the gallbladder meridian on the
temporal side of the head.

For correct manipulation, either a sitting or a dorsal position is
appropriate. The area should be routinely sterilized before insertion
of the needle. Number 30 Hwato needles of 0.30 mm in diameter
and 40 mm in will be obliquely inserted then parallelly pierced 25 to
35 mm deep, along the lines described above, for point prescription.
The acupuncture will be maintained for 30 minutes with rapid
twirling performed for 2 to 3 minutes once 10 minutes. after
withdrawing the needle, a dry sterilized cotton ball should be
pressed the puncture holes as quickly as possible to prevent
bleeding. The therapy will be given once a
Anti-tragus — the small prominence opposite the tragus, just above the ear canal.
1. Aphasia Quotient (AQ) of the Western Aphasia Battery (WAB)
Description:
The Aphasia Quotient (AQ) is a composite score derived from the Western Aphasia Battery (WAB), a standardized test used to evaluate the severity and type of aphasia. It measures various aspects of language performance including spontaneous speech, auditory comprehension, repetition, and naming.
Domains assessed include:
• Comprehension (understanding spoken language)
• Expression (verbal and non-verbal communication)
• Reading and writing skills
• Social communication and practical communication tasks
Speech and language therapy
• During a retained time of the scalp acupuncture therapy, the experimental group patients were Not receive Speech & Language Therapy.
Childhood Apraxia of Speech
Verbal apraxia (VA), including Childhood Apraxia of Speech (CAS) and related disorders, is a severe neurological speech-motor planning disorder that often goes unrecognized and untreated in early childhood. Many affected children struggle to produce correct sounds, syllables, and words, and some may require alternative communication methods. VA shares overlapping symptoms with autism spectrum disorders (ASD) and vitamin E deficiency,
including limb dyspraxia, hypotonia, and sensory integration issues. Low vitamin E and polyunsaturated fatty acid (PUFA) levels can contribute to neurological dysfunction, which may be improved with supplementation. This study investigates the effects of Omega-DEK plus L-carnitine in children aged 3–6 years with CAS over a 12-week open-label period, followed by an 8-week blinded trial comparing continued treatment versus placebo.
Conclusion
Acupuncture promotes recovery in post-stroke Aphasia and child hood Apraxia by regulating neurotransmitter systems, reducing excitotoxic neuronal injury, improving cerebral blood flow, and enhancing neuroplasticity. Through these combined cellular, molecular, and systemic effects, acupuncture facilitates the reconstruction of damaged language networks, leading to improved speech, comprehension, and overall neurological function.
Recovery outcomes: 32 patients of Post-Stroke Aphasia and 14 Child hood Apraxia patients received a standardized course of Acupuncture Therapy.
Primary outcomes: at the end of the treatment period 30 out of 46 patients 65.21% met the predefined criteria to recovery.
For further information: Website: www.fastb.ac.in | You Tube: Prof.Samiullah – F A S T Board