A study to analyze the effectiveness of Constraint Induced Movement Therapy and Robot Assisted Therapy in Improving Upper Limb Function of Patients with Hemiplegia: Dr.Utikonda Bhaskara Rao, M.P.T., Principal, Sarada College of Physiotherapy, Ongole, Andhra Pradesh, India; 1 Dr.Kurapati Madhava Reddy, Ph.D., D.Sc., Professor & Principal, Sri Lakshmi Institute of Medical Sciences College of Physiotherapy, Kavali, Andhra Pradesh, India.2
Background:
Stroke is a medical emergency which can cause permanent neurological damage or death. Human functions such as movement, sensation or emotions that were controlled by the affected area of the brain are lost or impaired. The severity of the loss of function varies according to the location and extent of the brain involved.
The World Health Organization (2005) defines stroke as the rapid development of clinical signs and symptoms of a focal neurological disturbance lasting more than 24 hours or leading to death with no apparent cause other than vascular origin. A stroke is the disturbance in blood supply, when blood vessel ruptured or blocked by a clot, which cuts off the oxygen supply and nutrients to the brain, causing damage to the brain tissue. Stroke is a clinical syndrome divided into two broad classifications such as ischemic stroke which is caused by sudden occlusion of arteries supplying the brain, either due to a thrombus at the site of occlusion or formed in another part of the circulation. It accounts for 50% to 85% of all strokes worldwide. A hemorrhagic stroke occurs due to injury to a blood vessel wall and formation of clot. It accounts for 15% of all strokes worldwide.
Worldwide stroke is the fourth leading cause of disability. According to the WHO (2015), each year 15 million people worldwide suffer from stroke. In that nearly 5 million people die and another 5 million people are left permanently disabled. It forecasts that disability-adjusted life years (DALYs) lost to stroke will rise from 38 million in 1990 to 61 million in 2020. The prevalence of new or recurrent stroke is nearly 750,000 in each year and above 4 million is living with the residual effects of stroke which includes paralysis and disability. In India, stroke is one of the leading causes of death and disability. The prevalence rate ranges from 84-262/100,000 in rural areas and 334-424/100,000 in urban areas. Stroke signified 1.2% of total deaths in India.
Stroke risk increases with various risk factors such as age, sex, race, family history, hypertension, extreme alcohol consumption, smoking, tobacco, lack of physical exercise, obesity, high blood cholesterol level, diabetes mellitus, earlier TIA and heart diseases. The aged population has less chance of recovering from paralysis and disability; males are more at risk than females and ratio in India is 7:1. The prevalence of stroke among men may be due to smoking and drinking as well as higher among menopausal women in India.
Rehabilitation programs are different in worldwide that most commonly, certain types like inpatient rehabilitation centers with acute care facilities, outpatient & home rehabilitation. In those rehabilitation programs they practice mobility, communication, ADLs and normal bowel and bladder patterns. Recent research has focused on techniques using robotics and constraint induced movement therapy.
Constraint Induced Movement Therapy (CIMT) is a form of rehabilitation therapy that improves upper extremity function in stroke and other central nervous system damage victim by increasing the practice of their affected upper limb. CIMT has been shown to be an effective method of stroke rehabilitation irrespective of the level of initial motor ability, amount of chronicity, amount of previous therapy, affected side of hemiparesis or infarct site. A consistent exclusion criterion for CIMT has been less voluntary wrist and finger extension in the affected hand.
Constraint Induced Movement Therapy (CIMT) is now being implemented by therapists to promote better compliance. IulyTreger, Lena Aidinof et al (2012) conducted a single-blinded randomized controlled trail study among 28 samples to assess the effectiveness of constraint induced movement therapy (CIMT) at loewenstein rehabilitation hospital, Israel. The CIMT group received 1 hour daily physical rehabilitation session and unaffected arm was restrained for 4 hours for 2 weeks. The control group received routine physical rehabilitation. The subjects were requested to perform the following tasks such as transfer pegs from a saucer to a pegboard, grasp, carry, and release a hard rubber ball and eating using a spoon to remove the jelly from the plate, bring it towards the mouth, and then place it on another plate with the affected hand for 30 seconds. The number of repetitions in each test was recorded as an outcome. Study results revealed that CIMT therapy group showed significantly greater changes in all 3 tests than control group.
Many researchers used constraint induced movement therapy (CIMT) program to recover upper extremity function. CIMT is an evidence- based program in an enriched environment to increase the use of the affected upper extremity. Many results recommended that CIMT may be a successful method of improving function and use of the affected arms of patients exhibiting learned non-use.
Robot-assisted therapy (RAT) offers intensive, repetitive, and goal-oriented training to help hemiplegic patients recover upper limb function by promoting neuroplasticity and improving motor control. While some studies show mixed results compared to conventional therapy, particularly in chronic stroke patients, RAT can enhance compliance and motivation through engaging, game-like interfaces. The effectiveness can depend on factors like robot intensity, training specifics, and the patient’s stage of recovery, with some evidence suggesting greater gains over longer periods or with higher intensity (He Wang et al 2025).Robots provide consistent, high-repetition movement practice that is often difficult to achieve with manual therapy alone (He Wang et al 2025).
Robotic devices to provide assistance or resistance during repetitive arm movements (Alex Pollock et al 2014); Allows for high-intensity, repetitive training, which is crucial for motor learning and recovery; It be customized to provide different levels of assistance and track performance and can incorporate virtual reality and gaming to improve motivation (Gert Kwakkel et al 2007).
A study by Fasoli et al. 2004 comprising 56 patients with subacute stroke reported that patients who received conventional therapy alone showed little improvement, whereas patients who received robotic training plus conventional therapy continued to improve in the latter half of the inpatient rehabilitation period. This means that robot-assisted therapy is effective for improving upper limb motor function in patients with subacute stroke. A study by Lo et al. 2010 recruited 127 chronic stroke patients reported that robot-assisted therapy and conventional therapy produced similar amounts of improvement after 12 weeks of treatment. However, after 36 weeks of therapy, the robot-assisted therapy achieved greater motor improvement than did conventional therapy. A study in patients with chronic stroke by Hsief et al. 2012 also found significantly greater improvement in upper limb motor function in the higher-intensity robot-assisted training group than in the control treatment group. In contrast, upper limb motor recovery did not differ significantly between the lower-intensity training group and the control group. These findings suggest that the intensity is the most important parameter of robot-assisted therapy for upper limb motor recovery in patients with chronic stroke.
In addition, studies in patients with subacute stroke suggested that patients who received additional robotic therapy showed greater improvements in ADL (Susan E Fasoli et al 2004 & Stefano Masiero et al 2007). However, trials in patients with chronic stroke demonstrated no additional improvement in ADL over conventional therapy. In summary, robot-assisted therapy for upper limb motor function provides an additional effect on ADL function only in patients with subacute stroke. Further studies may be needed to draw a definite conclusion about the effect of robot-assisted training on ADL in patients with chronic stroke (E Fasoli et al 2004).
Aims & Objectives:
A study to analyze the effectiveness of Constraint Induced Movement Therapy and Robot Assisted Therapy in Improving Upper Limb Function of Patients with Hemiplegia.
Method:
It is a quasi-experimental pre-test post-test control group design was selected to evaluate the effectiveness of Constraint Induced Movement Therapy and Robot Assisted Therapy in Improving Upper Limb Function of Patients with Hemiplegia on 60 subjects who fulfilled inclusion and exclusion criteria were selected by Non probability purposive sampling technique and among 60 patients, 30 patients were assigned in Group A treated with Robot Assisted Therapy and 30 patients were assigned to Group B treated with Constraint Induced Movement Therapy; the study was conducted at Physiotherapy outpatient department Sarada College of Physiotherapy, Ongole, Andhra Pradesh for a period of 2 weeks. The study was conducted by using Constraint induced movement therapy and Robot Assisted Therapy as Independent Variables and Level of upper extremity function as dependent Variables. The outcome was assessed using Demographic variables such of age, sex, education, working status, social habits, food habit, pre stroke exercise and supportive members of family; Clinical variables such as type of stroke, side affected, pre stroke dominant side and duration of stay in hospital; Motor activity log
used to assess the level of motor arm function. Motor activity log with observation checklist consists of 15 items to examine the amount and how well patients have used their affected arm. The answers were interpreted based on 6-point rating scale (0-5). The minimum and maximum scores were 0 and 150 respectively. Modified Sollerman hand grip function scale with observation checklist which consists of 10 items was used to assess hand grip function and the answers were interpreted based on 5-point rating scale (0-4). The minimum and maximum scores were 0 and 40 respectively.
Ethical clearance was obtained from the ethical committee of The Medicina Alternativa, The open International University for Complimentary Medicines (OIUCM) – Colombo, Sri Lanka. Prior to the commencement of the study, the purpose of the study was explained and a written informed consent was taken from all the participants.
60 Hemiplegic patients who fulfilled the inclusion criteria were selected for the study. Non probability purposive sampling technique was used to select 60 patients, 30 patients were assigned in Group A treated with Robot Assisted Therapy and 30 patients were assigned to Group B treated with Constraint Induced Movement Therapy. After self-introduction, the investigator explained the nature of the study and obtained written consent from the patients. The demographic and clinical variables were collected from the patients.
Pre-test level of upper extremity function was assessed through motor activity log and modified Sollerman hand grip function scale with observation checklist, among both the groups on first day of the study. Followed by, Robot Assisted Therapy was demonstrated in Group A patients and the patients were made to practice the same for 14 consecutive days and post-test was conducted on 14th day; and constraint induced movement therapy was demonstrated in Group B patients and the patients were made to practice the same for 14 consecutive days and post-test was conducted on 14th day. The non-affected arm of the patients of both the Groups was restrained with splint for 4 hours and affected arm was practiced with repeated activities such as peg board, transferring jelly with spoon, picking and transferring the nuts, grasping the smiley ball for 4 hours under the supervision of the researcher. Both the Groups received routine rehabilitation program.
Data was analyzed using descriptive and inferential statistics which are necessary to provide substantive summary by the results in relation to the objectives. Paired and unpaired ‘t’ test was used to evaluate the effectiveness of Robot Assisted therapy and constraint induced movement therapy on level of upper extremity function. Chi square test was used to find out the association between the pre and post-test level of upper extremity function among hemiplegic patients with selected demographic and clinical variables in both the groups.
Results:
The Frequency and percentage distribution on level of motor arm function among patients in RAT and CMIT group shows that in Group A pre-test most of the 26 (86.67%) patients had very poor motor arm function, 3 (10%) patients had poor motor arm function and 1 (3.33%) patient had fair motor arm function in RAT group. In post
test most of the 18 (60%) patients had very poor motor arm function, 10 (33.34%)
patients had poor motor arm function, 1 (3.33%) patient had fair and almost normal motor arm function. In CMIT group most of the 26 (86.67%) patients had very poor motor arm function and 4 (13.33%) patients had poor motor arm function in pre-test. 25 (83.34%) patients had very poor motor arm function, 4 (13.33%) patients had poor motor arm function and 1 (3.33%) patient had fair motor arm function in post-test.
The Frequency and percentage on level of hand grip function among patients
in RAT and CMIT group shows that in RAT group most of the 26 (86.67%) patients had very poor hand grip function, 3 (10%) patients had poor hand grip function and 1 (3.33%) patient had fair hand grip function in pre-test. Half of the 15 (50%) patients had very poor hand grip function, 13 (43.33%) patients had poor hand grip function and 2
(6.67%) patients had fair hand grip function in post-test. In CMIT group most of the 28 (93.33%) patients had very poor hand grip function and 2 (6.67%) patients had poor hand grip function in pre-test. 22 (73.33%) patients had very poor hand grip function and 8 (26.67%) patients had poor hand grip function in post-test.
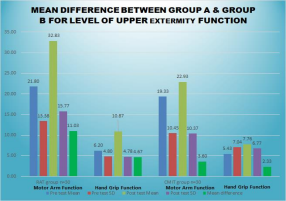
The Mean, Standard Deviation and Mean difference in Pre and Post test scores among patients in RAT and CMIT group in Pre test, the mean and standard deviation of motor arm function was 21.80 ± 13.38 in RAT group and 19.33 ± 10.45 in the CMIT group, whereas the mean and standard deviation of hand grip function was 6.20 ± 4.80 in RAT group and 5.43 ± 7.04 in the CMIT
group. In Post-test, the mean and standard deviation of motor arm function was 32.83 ± 15.77 in the RAT group and 22.93 ± 10.37 in the CMIT group, whereas the mean and standard deviation of hand grip function was 10.87 ± 4.78 in the RAT group and 7.76 ± 6.77 in the CMIT group. The mean difference of motor arm function was 11.03 and 3.60 and hand grip function was 4.67 and 2.33 in RAT and CMIT group respectively.
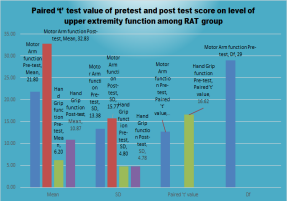
The results of the Paired ‘t’ test value of pretest and post test score on level of upper extremity function among RAT group – the calculated paired “t’ test value of motor arm function 12.67 was greater than the table value 2.46 at p<0.01 the calculated paired “t’ test value of hand grip function 16.62 was greater than the table value 2.46 which was highly significant at p<0.01. It reveals that the Robot Assisted therapy was effective in improving upper extremity function among hemiplegic patients. Hence, the hypothesis is retained.
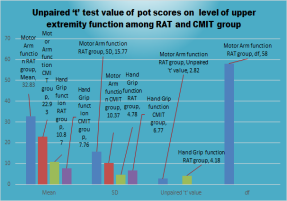
The results of the Un paired ‘t’ test value of pot scores on level of upper extremity function among RAT and CMIT group shows that the calculated unpaired ‘t’ test value of motor arm function 2.82 was greater than the table value 2.39 at p<o.01. The calculated unpaired ‘t’ value of hand grip function 4.18 was greater than the table value 2.39 which was highly significant at p<0.01. Hence it shows that Robot Assisted therapy was effective in improving level of upper extremity function for hemiplegic patients. Hence, the hypothesis is retained.
The results of the association between the pre and post-test scores on level of upper extremity function among patients and their selected variables in the RAT group show that in the RAT group, with regard to motor arm function there was a significant association found between working status and supportive members in the family whereas age, sex, education, social habit, food habit and pre stroke exercise were not associated at p< 0.05. In hand grip function, working status was found to be associated in post test score. Age, sex, education, social habit, food habit, pre stroke exercise and supportive members in family were not associated at p< 0.05. In the RAT group, with regard to motor arm function there was a significant association found between duration of stroke and duration of rehabilitation whereas type of stroke, affected arm and pre stroke dominant side were not associated at p< 0.05. In hand grip function duration of stroke and duration of rehabilitation was found to be associated in post test score. Type of stroke, affected arm and pre stroke dominant side were not associated at p< 0.05. Hence, the hypothesis is accepted for the above-mentioned variables such as working status, duration of stroke, duration of rehabilitation and supportive members in family and rejected for age, sex, education, social habit, food habit, type of stroke, affected arm and pre stroke dominant side.
Conclusion:
In conclusion, the present statistical analysis randomized study to analyze the effectiveness of Constraint Induced Movement Therapy and Robot Assisted Therapy in Improving Upper Limb Function of Patients with Hemiplegia showed that there was an improvement in level of upper extremity function after implementation of RAT in hemiplegic patients in Group A when compared to pre-test. Also, there was a difference in the post test scores on level of upper extremity function among ART Group and the CMIT Group. Thus, the results of the study concludes that Robot
Assisted Therapy is effective in Improving Upper Limb Function of Patients with Hemiplegia compared to patients treated with CMIT.
Keywords:
Constrained Induced Movement; Robot Assisted Therapy, Strength Training; hemiplegia.
References:
1. Devendra Singh, Bhagirath Pokhriyal, YM. Joshi and Vilasrao Kadam. (2012) Prevalence, risk factors and maintenance of Cerebral Stroke. International Journal of Research in Pharmacy and Chemistry. Vol.2/No.3, 866-870.
2. Ehab Mohamed Abd El-Kafy, Samah Attia Elshemy & Mohammed Saeed Alghamdi (2014) Effect of constraint-induced therapy on upper limb functions: A randomized control trial: Scandinavian Journal of Occupational Therapy Volume 21, 2014 – Issue 1
3. Eun-Cho Park, Seong-Gil Kim. (2015). The effects of virtual reality game exercise on balance and gait of the elderly patients. Journal of Physical Therapy Science. Vol 27/No 4, 1157-1159.
4. Gert Kwakkel, Boudewijn J Kollen, Hermano I Krebs: Effects of Robot-assisted therapy on upper limb recovery after stroke: A Systematic Review: Neurorehabil Neural Repair. 2007 Sep 17;22(2):111–121.
5. Gert Kwakkel. Boudewijn J. Kollen and Hermano I. Kreb (2008). Effect of robot assisted therapy on upper limb recovery after stroke. Neuro Rehabilitation and Neural repair. Vol.22, 111-21.
6. Han Gil Seo, Jaewon Beom, Byung-Mo Oh, Tai Ryoon Han: Effects of Robot assisted Upper Limb Training on Hemiplegic Patients: Brain Neurorehabil. 2014 Mar;7(1):39-47.
7. Harris JE, Eng JJ, Miller WC, Dawson AS. (2009). a self-administered Graded Repetitive Arm Supplementary Program (GRASP) improves arm function during inpatient stroke rehabilitation: a multi- site randomized controlled trial. Pubmed. Vol 40/No 6.
8. Hsieh YW, Wu CY, Lin KC, Yao G, Wu KY, Chang YJ. Dose-response relationship of robot-assisted stroke motor rehabilitation: the impact of initial motor status. Stroke. 2012;43:2729–2734.
9. He Wang, Xiaoxu Wu Yaning Li, Shaohong Yu: Efficacy of Robot-assisted Training on Upper Limb Motor Function After Stroke: A Systematic Review and Network Meta-analysis: Archives of Rehabilitation Research and Clinical Translation. Volume 7, Issue 1, March 2025, 100387.
10.Hwang CH, Seong JW, Son DS. Individual finger synchronized robot-assisted hand rehabilitation in subacute to chronic stroke: a prospective randomized clinical trial of efficacy. Clin Rehabil. 2012; 26:696–704.
11.JuHyung Park, Nayun Lee et al. (2015). Constraint-induced movement therapy for clients with chronic stroke: interrupted time series design. Journal of physical therapy science. Vol 27/No 3, 963-966.
12.Jin C, Chen Y, Ma Y (2025) Effectiveness of robot-assisted task-oriented training intervention for upper limb and daily living skills in stroke patients: A meta-analysis. PLoS ONE 20(1): e0316633.
13.Kenji Numata, Takashi murayama et al (2008) effects of constraint induced movement therapy (CIMT) on lower extremity hemiplegia due to a higher-motor area lesion. Brain injuries Vol 22/ No 11, 898-904.
14.Kwakkel, G., Veerbeek, J. M., van Wegen, E. E., and Wolf, S. L. (2015). Constraint induced movement therapy after stroke. Lancet Neurol. 14, 224–234. doi: 10.1016/S1474-4422(14)70160-7.
15.Luca Mirela Cristina, Daniela Matei, Bogdan Ignat and Cristian Dinu Popescu. (2015). Mirror therapy enhances upper extremity motor recovery in stroke patients. Acta Neurologica Belgica.84.
16.Lum PS, Godfrey SB, Brokaw EB, Holley RJ, Nichols D. Robotic approaches for rehabilitation of hand function after stroke. Am J Phys Med Rehabil. 2012;91: S242–S254.
17.Mahale Rutuja, Karajgi Asmita and Yardi Sujata. (2013). Effects of constraint induced movement therapy on upper extremity performance in chronic stroke patients. Indian journal of physiotherapy & occupation. Vol.7/No.4, 12-16.
18.Masashi Hosomi, Tetsuo Koyama et al. (2012) a method for constraint induced movement therapy: a supervised self-training protocol. Journal of stroke & cerebrovascular diseases.
19.Murali (2013). Effectiveness of Sensory Stimulation Program (SSP) on motor function and verbal response among stroke patients. Journal of Medical & Surgical Nursing. Vol.11/ Issue.2, 12.
20.Naylor CE. (2005). Constraint induced movement therapy for young children with hemiplegic cerebral palsy; a pilot study. Development Medicine and Child Neurology. Vol.47, 365-369.
21.Page, Stephen J, Sisto, Sue Ann PT, Levine and Peter BA. (2002). Constraint Induced Therapy in Chronic Stroke. American Journal of Physical Medicine & Rehabilitation. Vol.81/issue 1, 870-875.
22.Rogers MA, Evans WJ, Changes in skeletal muscle with aging: Training Exer Sport Sci. Rev. 1993; 21: 65 – 102 (Medline).
23.Siddharth Mishra and Jeba Chitra. (2014). Effect of Constraint Induced Movement Therapy (CIMT) for lower limb on weight bearing symmetry and balance in stroke patients. International Journal of Scientific Research. Vol.3 /issue. 6, 485-488.
24.Siebers A, Oberg U, Skargren E. (2010). The effect of Constraint Induced Movement Therapy on spasticity and motor function of the affected arm in patients with chronic stroke. Physiotherapy Can Help. Vol. 62, 388-396.85
25.Steven L. Wolf, Carolee J. Winstein. (2006). Effect of Constraint-Induced Movement Therapy on Upper Extremity Function 3 to 9 Months after Stroke: The EXCITE randomized clinical trial. The Journal of American; Medical Association. Vol. 296/No.17, 2095-2104
26.Susan E Fasoli , Hermano I Krebs, Mark Ferraro, Neville Hogan, Bruce T Volpe : Does shorter rehabilitation limit potential recovery poststroke? : Neurorehabil Neural Repair. 2004 Jun;18(2):88-94.
27.Thais Tavares Terranova , Marcel Simis , Artur César Aquino Santos, Fábio Marcon Alfieri , Marta Imamura, Felipe Fregni , Linamara Rizzo Battistella : Robot Assisted Therapy and Constraint-Induced Movement Therapy for Motor Recovery in Stroke: Results From a Randomized Clinical Trial. Front Neurorobot. 2021 Jul 21; 15:684019.
28.Thrane, G., Friborg, O., Anke, A., and Indredavik, B. (2014). A meta-analysis of constraint-induced movement therapy after stroke. J. Rehabil. Med. 46, 833–842.
29.Stefano Masiero , Andrea Celia, Giulio Rosati, Mario Armani : Robotic-assisted rehabilitation of the upper limb after acute stroke : Arch Phys Med Rehabil . 2007 Feb;88(2):142-9.
30.U. Ganapathy Sankar. (2013). Constraint Induced Movement Therapy (CIMT) for Children with Hemiplegic Cerebral Palsy to Improve Upper Extremity Function: Pilot Study. International Journal of Science and Research. Vol. 4/ Issue. 5, 3029- 3032.
31.Uswatte, Gitendra | Taub, Edwarda | Bowman, Mary H.a | Delgado, Adrianaa | Bryson, Camillea | Morris, David M.b | Mckay, Stacia | Barman, Joydipa | Mark, Victor W. : Rehabilitation of stroke patients with plegic hands: Randomized controlled trial of expanded Constraint-Induced Movement therapy: Restorative Neurology and Neuroscience, vol. 36, no. 2, pp. 225-244, 2018.
32.Wei-ming Zhang, Shuai yang. (2015). Effect of constraint- induced movement therapy on the activities of daily living (ADL) of patients with acute stroke. Chinese Journal of Contemporary neurology & Neurosurgery. Vol. 15/No.4